
“In people with skin of color, rosacea is often an unrecognized disorder,” remarked the authors of a 15-page study published in the Journal of the American Academy of Dermatology (JAAD). This statement challenges the previously held belief in medical literature that positioned rosacea as less common among people with darker skin tones.
To shed more light on the diagnostic barriers that may contribute to the underreporting and detection of rosacea in people of color, this MedDigest article takes a closer look at the common skin condition, which can severely disrupt quality of life.
In This Article: (7 min read⏱️)
🆕 What is Rosacea & How Common is it in People of Color?
🧑 Causes & Signs of Rosacea in Darker Skin Tones
🩹 How is Rosacea Different from Acne?
🧑⚕️ Diagnosing & Treating Rosacea in Patients of Color

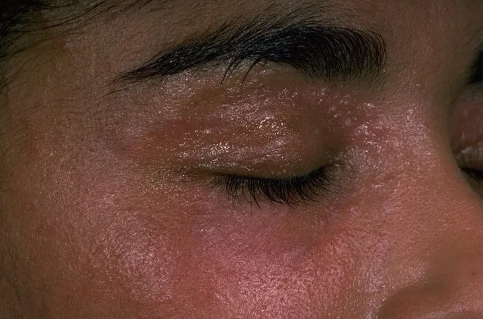
Rosacea mainly affects the face. Tell-tale skin redness may not be easily discernible in darker skin tones.
What is Rosacea?
Rosacea is a skin condition that mainly affects the face. You may see flushing, persistent color (red, violet, or brown), acne-like breakouts, or visible blood vessels (telangiectasia) on your face. Some people may have eye (ocular) manifestations such as conjunctival injection (redness), ocular irritation and tearing, or thickening skin (also called phymatous changes).
People with lighter skin tones often develop redness, and people with darker skin tones may see a brown or violet color on their face.

Rosacea in people with lighter skin tones often shows redness (left). Rosacea in people with darker skin tones may see a brown or violet color on their face (right).
How Common is Rosacea Among People of Color?
Rosacea is infrequently reported among nonwhite populations worldwide, but difficulty detecting its characteristics in darker skin might be leading to its underdiagnosis.
In a 1993-2010 US National Ambulatory Medical Care Survey on the racial/ethnic distribution of patients with rosacea, it was found that 2% of rosacea patients were black, 2.3% were Asian or Pacific Islander, and 3.9% were Hispanic or Latino.
Globally, the reported prevalence of rosacea in people with skin of color has varied, with estimates as high as 40 million cases and rates up to 10%. Despite these estimates, epidemiologic reports often depict rosacea as less prevalent among people of color. In fact, this might be due to underreporting and underdiagnosing rosacea in populations with skin of color because of the difficulty of discerning erythema (redness) and telangiectasia (visibly tiny blood vessels) in dark skin.
Ocular (eye) signs of rosacea may be important clues in patients with skin of color.
What Causes Rosacea?
Regardless of skin color, the exact cause of Rosacea is not fully understood. Dysregulation of the innate immune system, commensal microorganisms, ultraviolet radiation exposure, vascular hyperreactivity, genetic and environmental factors have all been thought to play a part in the development of Rosacea.
What are the Signs of Rosacea in Colored Skin?
If you have a darker skin tone, the American Academy of Dermatologist recommends that you make a dermatology appointment if you notice any of the following on your face:
-
A warm feeling most of the time
-
Dry, swollen skin and patches of darker skin
-
A dusky brown discoloration to your skin
-
Acne-like breakouts that acne treatment won’t clear
-
Yellowish-brown, hard bumps around your mouth, eyes, or both
-
Burning or stinging when you apply skin care products
-
Swelling and thickening skin on your nose, cheeks, chin, or forehead

Avoiding rosacea triggers prevents flares & improves quality of life.
Things that Trigger Rosacea Flare
Rosacea is a condition that flares and then calms down. Your dermatologist may call these “exacerbations” (flares) and “remissions” (calms down).
If you have rosacea, you may notice that it worsens at certain times of the year or when you do certain things. In the winter, your face may feel raw and irritated when you’re outside on a cold, windy day. After drinking a glass of red wine, your face may feel hot and uncomfortable.
Anything that worsens your rosacea is called a trigger. Many things can be a trigger, and triggers tend to vary from person to person. Some of the most common rosacea triggers are:
📌Stress
📌Sunlight
📌Alcohol, especially red wine
📌Wind
📌Heat
📌Spicy foods
📌Hot beverages
📌Exercise
📌Some skin care or hair care products

Rosacea differs from acne. Telling them apart is important.
How is Rosacea Different from Acne?
Do you have acne-like breakouts that nothing seems to clear? Are you bothered by frequent sunburns on your face? Does your face often feel warm? When you apply certain skin care products, does your skin sting or burn? If you answered “yes” to these questions, you might have rosacea.
In Acne, pustules and erythematous papules on face and upper trunk, usually accompanied by open and closed comedones and no telangiectasia, with initial onset typically occurring in adolescence and young adulthood.
To find out what’s causing your skin condition, the American Academy of Dermatology recommends that you see a board-certified dermatologist.

Diagnosing Rosacea in Darker Skin Tones
The diagnosis of rosacea is made based on clinical assessment. Given that erythema and telangiectasia are more difficult to visualize in individuals of darker skin tone, there is a risk of misdiagnosis.
Therefore, clinicians should pay greater attention to other elements of the patient’s history. Features such as a history of facial stinging or burning sensation, experiences of facial flushing, a history of acne diagnosis and failed acne treatments, can all help with diagnosis in patients with highly pigmented skin.
The absence of comedones in the presence of inflammatory papules and pustules continues to be a differentiating clinical feature when compared to acne vulgaris.
Dermoscopy may help with being able to identify telangiectasia by differentiating skin pigment versus blood vessels.
Skin biopsies are rarely indicated in diagnosing rosacea as the cutaneous histopathological findings are non-specific. A skin biopsy may be used to rule out other disorders or to support a diagnosis for granulomatous rosacea.

Early treatment of rosacea improves quality of life.
How is Rosacea Treated in Patients of Color?
Rosacea treatment is similar for all patients, regardless of skin color.
Rosacea treatment involves a combination of non-pharmacologic interventions, topical therapies, systemic therapies, and in some cases, laser or light-based treatments. The choice of treatment depends on the subtype and severity of the disease, as well as the patient’s individual tolerance and response to therapy.
Non-pharmacologic interventions
Skin care: Daily use of water-based broad-spectrum sunscreen with a sun protection factor > 30, daily application of fragrance-free moisturizers, and twice-daily facial cleansing should reduce symptoms in patients with rosacea.
Patient education: Educating patients about trigger avoidance and skin care techniques such as moisturizing and sun protection are important first steps in managing rosacea.
Topical therapies
First-line options: Ivermectin, metronidazole, or azelaic acid are recommended as first-line topical treatment options for patients with papulopustular rosacea.
Other options: Topical brimonidine or oxymetazoline may be considered for patients where the main presenting feature is facial erythema. Topical minocycline foam may be considered for patients with papulopustular rosacea.
Systemic therapies
Antibiotic therapy: Low-dose doxycycline (40 mg) is recommended as first-line systemic therapy for patients with moderate-to-severe rosacea with papules and pustules.
Other oral antibiotics such as azithromycin, clarithromycin, doxycycline, erythromycin, lymecycline, and oxytetracycline may be considered for more severe papulopustular rosacea.
Beta-blockers: Oral propranolol may be considered for patients where the main presenting feature is transient facial erythema (flushing).
Isotretinoin: Low-dose isotretinoin has been found effective for difficult-to-treat papulopustular rosacea.
Laser and intense pulsed light therapy
Pulsed dye laser, Nd-YAG laser, or intense pulse light may be considered for patients where the main presenting feature is persistent facial erythema.
Bottom Line
The treatment of rosacea is multifaceted and should be tailored to the individual patient’s needs and disease characteristics. It is important to discuss the potential for irritancy of different products and formulations before prescribing the topical agent.